 We're all familiar with the appearance of osseous hemangiomas of the vertebral bodies -- osseous hemangioma is common in the axial skeleton, with 75% occurring in the spine and calvaria. Twenty percent of cases occur in the scapula, ribs, clavicle, and pelvic bones, and involvement of the long bones is rare. Osseous hemangiomas occur in young adults, with a mean age of ~30 years, and are more common in women. The majority (90%) of patients are symptomatic. 10% of patients present with a pathological fracture.
We're all familiar with the appearance of osseous hemangiomas of the vertebral bodies -- osseous hemangioma is common in the axial skeleton, with 75% occurring in the spine and calvaria. Twenty percent of cases occur in the scapula, ribs, clavicle, and pelvic bones, and involvement of the long bones is rare. Osseous hemangiomas occur in young adults, with a mean age of ~30 years, and are more common in women. The majority (90%) of patients are symptomatic. 10% of patients present with a pathological fracture.
In the long bones, osseous hemangiomas can be classified as medullary (~50%), periosteal (~35%), and intracortical (~15%).
Medullary osseous hemangiomas occur most commonly in the diaphysis (48% of cases), with metadiaphyseal (30%), metaphyseal (12%), metaepiphyseal (4%), epimetadiaphyseal (3%) and epiphyseal (1%) lesions occurring less commonly. On radiographs, medullary lesions can have corduroy and radiating trabecular thickening similar to those seen in the vertebral bodies and skull, respectively, but this is an uncommon presentation. A more common appearance is a bubbly pattern of bone lysis that creates a honeycomb, lattice-like, or "hole-within-hole" appearance. This bone lysis can appear as linear and circular densities on radiographs, representing vascular channels seen longitudinally and en face, respectively. The appearance can mimic that of lymphoma, osteomyelitis and metastatic disease.
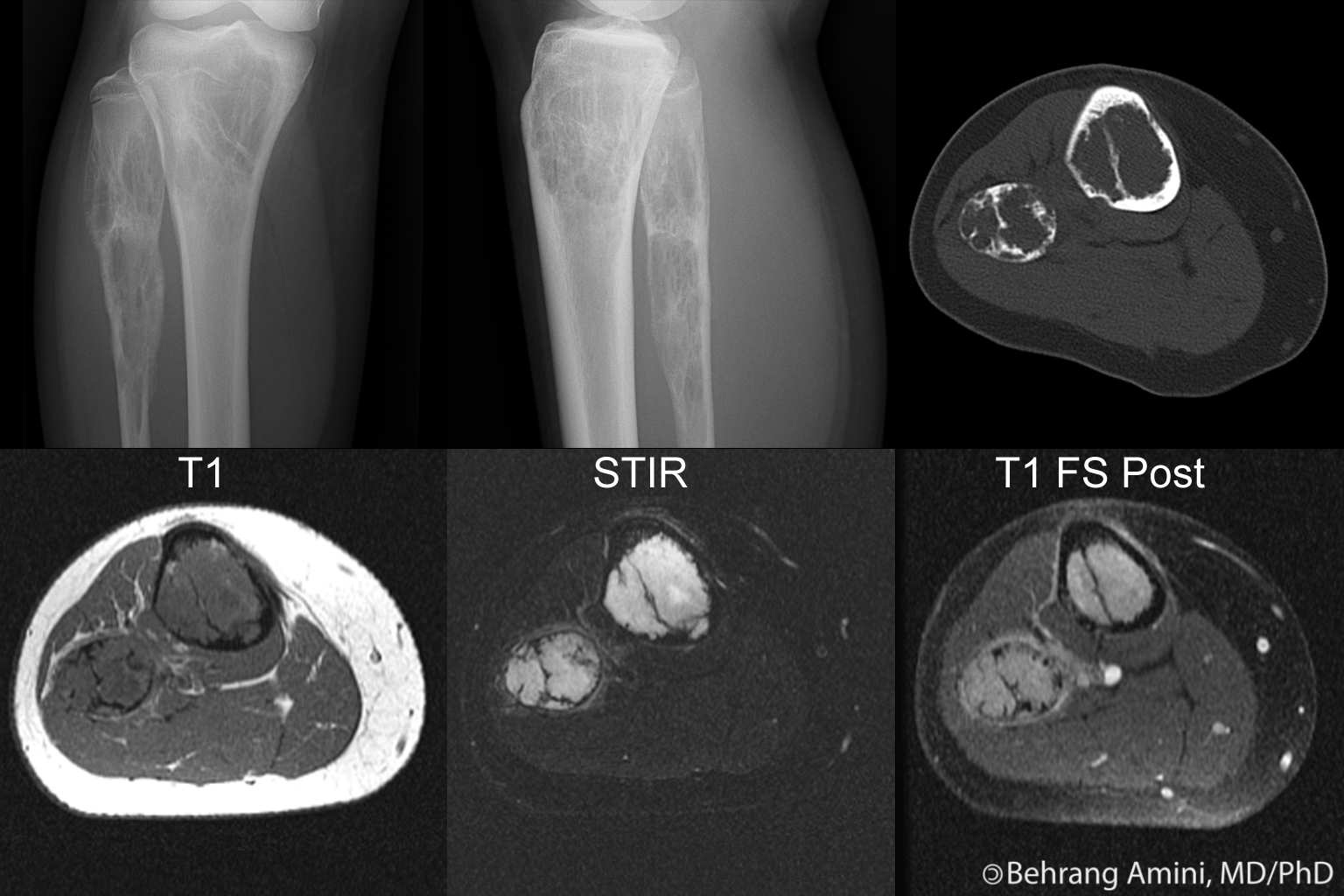
On CT, medullary hemangiomas appear as expansile lytic areas surrounded by coarse trabecular bone. A "polka dot" appearance, when seen, can suggest the diagnosis.
On MRI, the vascular channels are hypointense on T1-weighted images and hypointense to very hyperintense on T2-weighted images depending on the speed of blood flow. The trabeculations may be seen as areas of low signal.
Less common radiographic appearances include punched-out lucencies that can mimic metastatic disease or multiple myeloma; large, lytic, lesions with sclerotic borders that can mimic giant cell tumor, unicameral or aneurysmal bone cyst, or fibrous dysplasia; and permeative pattern that can mimic multiple myeloma, metastatic carcinoma, lymphoma, or Ewing sarcoma. In these cases, the rarity of osseous hemangioma would preclude its inclusion in the differential diagnosis.
Periosteal and intracortical lesions also occur most commonly in the diaphyis (~75%), wit the anterior tibial diaphysis being a common location. Metadiaphyseal (~15%) and metaphyseal (~10%) lesions can also be seen. On radiographs, they present as small, well-defined lytic lesions that may also be associated with cortical thickening and/or periosteal reaction. The differential diagnosis includes stress fracture, osteoid osteoma, or cortical abscess.
On MRI, intracortical lesions appear as increased signal within the normally dark cortex.
Should be considered in the differential diagnosis of fat-containing bone lesions.
References
- Chawla A, Singrakhia M, Maheshwari M, Modi N, Parmar H. Intraosseous haemangioma of the proximal femur: imaging findings. Br J Radiol. 2006 Aug;79(944):e64-6.
- Greenspan A, Jundt G, Remagen W. Vascular Lesions. In Differential Diagnosis of Orthopaedic Oncology, 2nd Edition. 2007 Lippincott Williams & Wilkins; pp 366-367.
- Kaleem Z, Kyriakos M, Totty WG. Solitary skeletal hemangioma of the extremities. Skeletal Radiol. 2000 Sep;29(9):502-13.
- Levine SM, Lambiase RE, Petchprapa CN. Cortical lesions of the tibia: characteristic appearances at conventional radiography. Radiographics. 2003 Jan-Feb;23(1):157-77.
- Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, Smith WS. From the archives of the AFIP. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics. 1995 Jul;15(4):893-917.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.