 If lateral views of the ankle are obliqued along the horizontal plane, the talar domes no longer overlap. Similarly, the medial (black arrows) and lateral (pink arrows) inferior margins of the talus can separate and fool you into calling a fracture. The posterior margin (white arrow) can also simulate a cortical defect.
If lateral views of the ankle are obliqued along the horizontal plane, the talar domes no longer overlap. Similarly, the medial (black arrows) and lateral (pink arrows) inferior margins of the talus can separate and fool you into calling a fracture. The posterior margin (white arrow) can also simulate a cortical defect.
Tuesday, November 30, 2010
Pseudofracture of the Talus
If lateral views of the ankle are obliqued along the horizontal plane, the talar domes no longer overlap. Similarly, the medial (black arrows) and lateral (pink arrows) inferior margins of the talus can separate and fool you into calling a fracture. The posterior margin (white arrow) can also simulate a cortical defect.
Monday, November 29, 2010
Coned Cecum
A cone-shaped cecum refers to a narrowed and thick-walled cecum. Differential considerations include:
- Tuberculosis: Terminal ileum can be involved.
- Crohn disease: Terminal ileum is involved.
- Amebiasis: Terminal ileum is not involved. Can cause ulcerations with skip lesions.
- Ulcerative colitis: Dilated terminal ileum (backwash ileitis)
- Typhlitis
- Lymphoma
- Cecal carcinoma
- Radiation therapy
- Metastases
References
- Silva AC, Beaty SD, Hara AK, Fletcher JG, Fidler JL, Menias CO, Johnson CD. Spectrum of normal and abnormal CT appearances of the ileocecal valve and cecum with endoscopic and surgical correlation. Radiographics. 2007 Jul-Aug;27(4):1039-54.
- Thoeni RF, Cello JP. CT imaging of colitis. Radiology. 2006 Sep;240(3):623-38
Sunday, November 28, 2010
Subependymal Giant Cell Astrocytoma
 Subependymal giant cell astrocytomas (SEGAs) are the most common cerebral neoplasm in patients with tuberous sclerosis, being found in up to 15% of patients. They are thought to arise from subependymal nodules in the ventricular wall.
Subependymal giant cell astrocytomas (SEGAs) are the most common cerebral neoplasm in patients with tuberous sclerosis, being found in up to 15% of patients. They are thought to arise from subependymal nodules in the ventricular wall.
Subependymal giant cell astrocytomas are almost always found near the foramen of Monro, are slowly-growing, and are WHO grade I tumors. The majority of cases occur during the first two decades of life.
CT reveals a heterogeneously low to iso attenuation lesion with or without calcifications in the region of the foramen of Monro with avid and heterogeneous enhancement. T1- and T2-weighted images reveal the mass to be hypo- to isointense to gray matter. The mass is heterogeneously hyperintense on FLAIR images. T2* images may show punctate hypointensities corresponding to calcium. Similar to CT, there is avid enhancement.
Differential considerations include:
- Subependymoma: Most common location is the lower fourth ventricle and the frontal horns of the lateral ventricles. Found in older patients. Typically none to mild enhancement, which is more commonly seen in fourth ventricle subependymomas
- Central neurocytoma: May also arise near foramen of Monro or septum pellucidum. Found in young adults (SEGAs typically occur during the first two decades). Look for necrosis and cyst formation.
- Choroid plexus tumors: For example, papillomas or carcinomas. These demonstrate avid enhancement and may have seeding via cerebrospinal fluid. The latter is not seen with subependymal giant cell astrocytoma. In addition, carcinomas may invade the brain parenchyma
- Astrocytoma: May arise from the fornices of the septum pellucidum or the medial basal ganglia. Enhancement is variable and calcifications are rare.
- Germinoma: These often arise near the third ventricle, seed via the cerebrospinal fluid.
References
- Koeller KK, Sandberg GD. Cerebral intraventricular neoplasms: radiologic-pathologic correlation. Radiographics. 2002 Nov-Dec;22(6):1473-505.
- Hedlund GL. Subependymal Giant Cell Astrocytoma. STATdx. Amirsys, Inc.
Saturday, November 27, 2010
Radiographic Deteremination of Distal Radioulnar Joint Dislocation
Distal radioulnar joint (DRUJ) dislocation can be caused by fractures of the distal radius (most common cause) and distal ulna (e.g., styloid process) and injury to the triangular fibrocartilage complex, dorsal and palmar radioulnar ligaments, interosseous membrane, or joint capsule. Radiography is generally unreliable for diagnosis because of the difficulty in obtaining standard views, but recognition of typical findings and associated injuries is nonetheless important.
Frontal radiographs may reveal an avulsion fracture of the triangular fibrocartilage complex, an ulnar styloid fracture or nonunion, and shortening of the radius. Increased overlap between the radius and ulna indicates volar ulnar dislocation, while increased distance between the sigmoid notch and the distal ulna indicates dorsal ulnar dislocation (more common).
A true lateral radiograph of the wrist with the forearm in neutral rotation (i.e., without supination or pronation) is needed. With true lateral views, the pisoscaphoid distance (between anterior margins of the scaphoid and pisiform) and the radioulnar distance (between the posterior margins of the radius and ulna) can be measured in both wrists. The difference between the two pisoscaphoid distances should be less than 3 mm and the difference between the two radioulnar distances should be less than 5 mm. A radioulnar difference of 6 mm or more is diagnostic of dislocation and a radioulnar difference between 5 mm and 6 mm is considered borderline, requiring additional imaging.
Frontal radiographs may reveal an avulsion fracture of the triangular fibrocartilage complex, an ulnar styloid fracture or nonunion, and shortening of the radius. Increased overlap between the radius and ulna indicates volar ulnar dislocation, while increased distance between the sigmoid notch and the distal ulna indicates dorsal ulnar dislocation (more common).
A true lateral radiograph of the wrist with the forearm in neutral rotation (i.e., without supination or pronation) is needed. With true lateral views, the pisoscaphoid distance (between anterior margins of the scaphoid and pisiform) and the radioulnar distance (between the posterior margins of the radius and ulna) can be measured in both wrists. The difference between the two pisoscaphoid distances should be less than 3 mm and the difference between the two radioulnar distances should be less than 5 mm. A radioulnar difference of 6 mm or more is diagnostic of dislocation and a radioulnar difference between 5 mm and 6 mm is considered borderline, requiring additional imaging.
References
- Tsai PC, Paksima N. The distal radioulnar joint. Bull NYU Hosp Jt Dis. 2009;67(1):90-6.
- Nakamura R, Horii E, Imaeda T, Tsunoda K, Nakao E.Distal radioulnar joint subluxation and dislocation diagnosed by standard roentgenography. Skeletal Radiol. 1995 Feb;24(2):91-4.
Friday, November 26, 2010
Coracoclavicular Joint
 The coracoclavicular joint is a normal variant, where there is a diarthrosis between the conoid tubercle of the clavicle and the superior surface of the horizontal part of the coracoid process of the scapula. The coracoclavicular joint can cause shoulder pain in the setting of arthritis. The images above show radiographs and axial and coronal CTs of a left coracoclavicular joint. The color image is a SPECT/CT fusion of a bone scan obtained for an unrelated condition, showing no evidence of abnormal uptake.
The coracoclavicular joint is a normal variant, where there is a diarthrosis between the conoid tubercle of the clavicle and the superior surface of the horizontal part of the coracoid process of the scapula. The coracoclavicular joint can cause shoulder pain in the setting of arthritis. The images above show radiographs and axial and coronal CTs of a left coracoclavicular joint. The color image is a SPECT/CT fusion of a bone scan obtained for an unrelated condition, showing no evidence of abnormal uptake.
References
Hall FJ. Coracoclavicular Joint. Br Med J. 1950 Apr 1;1(4656):766-768.Thursday, November 25, 2010
Amputation Stump Neuroma
 Amputation stump neuromas are a common cause of stump pain and can be classified as terminal or spindle neuromas. Terminal neuromas are formed as distal axons in a transected nerve grow in an attempt to reunite with non-existent distal axons cells and form a bulbous mass. Spindle neuromas, on the other hand, are not located at the transected nerve, but at a peripheral nerve that has been exposed to microtrauma from stretching or compression by local scar tissue.
Amputation stump neuromas are a common cause of stump pain and can be classified as terminal or spindle neuromas. Terminal neuromas are formed as distal axons in a transected nerve grow in an attempt to reunite with non-existent distal axons cells and form a bulbous mass. Spindle neuromas, on the other hand, are not located at the transected nerve, but at a peripheral nerve that has been exposed to microtrauma from stretching or compression by local scar tissue.
Amputation stump neuromas usually present within a year of surgery and can continue to enlarge for 3 years.
MRI is the imaging modality of choice for detection of a neuroma and differentiation of soft tissue stump mass from tumor recurrence. Stump neuromas have low signal intensity on T1-weighted images and intermediate-to-high signal intensity on T2-weighted images. They demonstrate variable contrast enhancement. Ultrasound can also be used for diagnosis of neuromas, which classically appear as oval-shaped, hypoechoic masses that are contiguous with a nerve. The margins of the mass can be well-defined or irregular.
References
- Ernberg LA, Adler RS, Lane J. Ultrasound in the detection and treatment of a painful stump neuroma. Skeletal Radiol. 2003 May;32(5):306-9.
- Henrot P, Stines J, Walter F, Martinet N, Paysant J, Blum A. Imaging of the painful lower limb stump. Radiographics. 2000 Oct;20 Spec No:S219-35.
Wednesday, November 24, 2010
Pseudodefect of the Capitulum
The capitulum narrows distally, where there is a change in contour at the junction of the capitulum anteriorly with the lateral epicondyle posteriorly. This change in contour at the posterolateral margin can look like an osteochondral defect and is referred to as the "pseudodefect of the capitulum"
Coronal images through the posterior capitulum and sagittal images through the lateral epicondyle can demonstrate this apparent defect.
Real osteochondral defects can be differentiated from this pseudodefect by the presence of flattening and deformity of the anterior surface of the capitulum, which is normally smooth. In addition, acute osteochondral defects are usually accompanied by bone marrow signal abnormalities.
Coronal images through the posterior capitulum and sagittal images through the lateral epicondyle can demonstrate this apparent defect.
Real osteochondral defects can be differentiated from this pseudodefect by the presence of flattening and deformity of the anterior surface of the capitulum, which is normally smooth. In addition, acute osteochondral defects are usually accompanied by bone marrow signal abnormalities.
References
Hughes T, Chung CB. Chapter 12. In Chung CB and Steinbach LS. MRI of the Upper Extremity: Shoulder, Elbow, Wrist, and Hand. Lippincott Williams & Wilkins. 2010. pp 462.Tuesday, November 23, 2010
Proximal Femoral Focal Deficiency
 Proximal femoral focal deficiency refers to congenital absence or hypoplasia of the proximal femur. It is characterized by a short femur with proximal deficiency and varus deformity of the femoral neck.
The Aitken classification divides proximal femoral focal deficiency into four categories. The Amstutz classification subdivides Aitken class A into Amstutz types 1 and 2. Amstutz types 3, 4, and 5 represent Aitken classes B, C, and D, respectively.
Proximal femoral focal deficiency refers to congenital absence or hypoplasia of the proximal femur. It is characterized by a short femur with proximal deficiency and varus deformity of the femoral neck.
The Aitken classification divides proximal femoral focal deficiency into four categories. The Amstutz classification subdivides Aitken class A into Amstutz types 1 and 2. Amstutz types 3, 4, and 5 represent Aitken classes B, C, and D, respectively.
- Class A: Short femur with coxa vara. Well-formed acetabulum.
- Amstutz type 1: Cartilaginous femoral neck.
- Amstutz type 2: Pseudoarthrosis at the femoral neck.
- Class B: No connection between the femoral head and shaft.
- Class C: Dysplastic acetabulum. Small or absent femoral head not adjoined to the femoral shaft.
- Class D: Both the acetabulum and femoral head are absent.
References
- Hillmann JS, Mesgarzadeh M, Revesz G, Bonakdarpour A, Clancy M, Betz RR. Proximal femoral focal deficiency: radiologic analysis of 49 cases. Radiology. 1987 Dec;165(3):769-73.
- Maldjian C, Patel TY, Klein RM, Smith RC. Efficacy of MRI in classifying proximal focal femoral deficiency. Skeletal Radiol. 2007 Mar;36(3):215-20.
Monday, November 22, 2010
Bipartite Sesamoid vs Fractured Sesamoid
 Distinguishing a bipartite hallux sesamoid from a fractured hallux sesamoid can be challenging. While the clinician can easily tell by physical examination, the typical history of "rule out pain" that accompanies the majority of radiograph requisitions contains no helpful clues.
Distinguishing a bipartite hallux sesamoid from a fractured hallux sesamoid can be challenging. While the clinician can easily tell by physical examination, the typical history of "rule out pain" that accompanies the majority of radiograph requisitions contains no helpful clues.
Several findings can help differentiate a bipartite hallux sesamoid from a fractured medial hallux sesamoid:
- Size: A medial sesamoid with a fracture is slightly larger than the lateral sesamoid, whereas a bipartite sesamoid is much larger.
- Cortication: Fractures have sharp, radiolucent, uncorticated lines, while bipartite sesamoids have two corticated fragments.
- Fit: The fragments of a fractured sesamoid often fit into each other, while the components of a bipartite sesamoid do not.
References
Mellado JM, Ramos A, Salvadó E, Camins A, Danús M, Saurí A. Accessory ossicles and sesamoid bones of the ankle and foot: imaging findings, clinical significance and differential diagnosis. Eur Radiol. 2003 Dec;13 Suppl 4:L164-77.Sunday, November 21, 2010
Ankle Effusions and Trauma
 The size of an ankle effusion following trauma can be used to suggest an underlying fracture. The effusion is measured as follows: Imaginary lines (white) are drawn parallel to the tibial shaft and tangential to the effusion margins at level of ankle joint. Another set of lines are drawn parallel to the first at edge of the articular surface of the tibia (dashed line). The distances between these two sets of lines are added. An ankle effusion >e; 13 mm has a positive predictive value of 80% for
occult fracture and is suggested as a reasonable threshold to prompt additional imaging.
The size of an ankle effusion following trauma can be used to suggest an underlying fracture. The effusion is measured as follows: Imaginary lines (white) are drawn parallel to the tibial shaft and tangential to the effusion margins at level of ankle joint. Another set of lines are drawn parallel to the first at edge of the articular surface of the tibia (dashed line). The distances between these two sets of lines are added. An ankle effusion >e; 13 mm has a positive predictive value of 80% for
occult fracture and is suggested as a reasonable threshold to prompt additional imaging.
References
Clark TW, Janzen DL, Ho K, Grunfeld A, Connell DG. Detection of radiographically occult ankle fractures following acute trauma: positive predictive value of an ankle effusion. AJR Am J Roentgenol. 1995 May;164(5):1185-9.Saturday, November 20, 2010
Os Subtibiale
 The os subtibiale is an uncommon accessory ossicle distal and posterior to the medial malleolus that is seen in less than 1% of the population. It is thought to represent an unfused epiphyseal ossification center related to the posterior colliculus of the medial malleolus.
The os subtibiale is an uncommon accessory ossicle distal and posterior to the medial malleolus that is seen in less than 1% of the population. It is thought to represent an unfused epiphyseal ossification center related to the posterior colliculus of the medial malleolus.
References
- Coral A. The radiology of skeletal elements in the subtibial region: incidence and significance. Skeletal Radiol. 1987;16(4):298-303.
- Coral A. Os subtibiale mistaken for a recent fracture. Br Med J (Clin Res Ed). 1986 Jun 14;292(6535):1571-2.
- Lapidus PW. OS SUBTIBIALE: Inconstant Bone Over the Tip of the Medial Malleolus. J Bone Joint Surg Am. 1933;15:766-771.
Friday, November 19, 2010
Varus instability of the Elbow
 Varus instability of the elbow is caused by disruption of the lateral collateral ligament complex, which includes the radial collateral ligament and lateral ulnar collateral ligament.
Varus instability of the elbow is caused by disruption of the lateral collateral ligament complex, which includes the radial collateral ligament and lateral ulnar collateral ligament.
The lateral collateral ligamentous complex consists of the radial collateral ligament (RCL, blue), lateral ulnar collateral ligament (LUCL, pink), and the annular ligament (AL, yellow).
The radial collateral ligament (RCL, blue) originates on the lateral epicondyle and inserts on the annular ligament. Because of this attachment, injury to the radial collateral ligament may be associated with injury to the annular ligament and vice versa.
The lateral ulnar collateral ligament (LUCL, pink) originates on the lateral epicondyle, passes along the posterolateral margin of the radial head, blends with fibers of the annular ligament, and inserts on the supinator crest of the ulna (SC).
The annular ligament originates from the anterior and posterior margins of the radial notch and surrounds the radial head. It is the primary stabilizer of the proximal radioulnar joint.
The image above shows a tear of the radial collateral ligament (blue arrow) and an intact lateral ulnar collateral ligament (pink arrow). A partial tear of the common extensor tendon is also present (white arrow).
The mechanism of injury in cases of varus instability is force to the medial side of the elbow, causing compression medially and stress applied to the radial collateral ligament. The etiology is usually trauma, but chronic stress, such as from crutches, has also been implicated.
References
Chung CB. Chapter 10. In Chung CB and Steinbach LS. MRI of the Upper Extremity: Shoulder, Elbow, Wrist, and Hand. Lippincott Williams & Wilkins. 2010. pp 426-427.Thursday, November 18, 2010
Accessory Sacroiliac Joint
 10% - 30% of the population has an accessory sacroiliac articulation between the posterior superior iliac spine and the lateral sacral crest at the level of the S2 foramen. These most commonly represent fibrocartilagenous connections that develop in response to weight bearing, but may also be present congenitally and represent true joints.
10% - 30% of the population has an accessory sacroiliac articulation between the posterior superior iliac spine and the lateral sacral crest at the level of the S2 foramen. These most commonly represent fibrocartilagenous connections that develop in response to weight bearing, but may also be present congenitally and represent true joints.
Here we see bilateral accessory sacroiliac joints (arrows) between the posterior superior iliac spine and the lateral sacral crest at the level of the S2 foramen.
References
Ehara S, el-Khoury GY, Bergman RA. The accessory sacroiliac joint: a common anatomic variant. AJR Am J Roentgenol. 1988 Apr;150(4):857-9.Wednesday, November 17, 2010
Congenital Dislocation of the Radial Head
Congenital dislocation of the radial head is the most common congenital elbow abnormality and usually occurs in association with other conditions (60% of the time), but can also occur in isolation. The more common associated conditions include lower extremity anomalies, scoliosis, mental retardation, and nail patella and Klippel-Feil syndromes.
The majority of radial head dislocations are posterior (65% of cases), followed by anterior (~15%) and lateral (~15%). Patients are usually asymptomatic in childhood, but may develop pain in adolescence.
The constellation of findings is now believed to be triggered by failure of development of a normal capitulum, which deprives the developing radial head of the contact pressure required for normal development and results in malformation of the radiocapitellar joint. This, in turn, results in altered biomechanics at the proximal radioulnar joint and abnormal development of the ulna.
The majority of radial head dislocations are posterior (65% of cases), followed by anterior (~15%) and lateral (~15%). Patients are usually asymptomatic in childhood, but may develop pain in adolescence.
The constellation of findings is now believed to be triggered by failure of development of a normal capitulum, which deprives the developing radial head of the contact pressure required for normal development and results in malformation of the radiocapitellar joint. This, in turn, results in altered biomechanics at the proximal radioulnar joint and abnormal development of the ulna.
- Capitulum: Hypoplastic and flattened
- Radius: Domed radial head articular surface.
- Ulna: Severely bowed and relatively short in relation to the radius. Negative ulnar variance at the wrist.
- Humerus: Mechanical erosion distally at pseudoarticulation with the dislocated radial head.
References
Hughes T and Chung CB. Chapter 12. In Chung CB and Steinbach LS. MRI of the Upper Extremity: Shoulder, Elbow, Wrist, and Hand. Lippincott Williams & Wilkins. 2010. pp 487-488.Tuesday, November 16, 2010
Cubital Tunnel
 The cubital tunnel is located posterior to the medial epicondyle and contains the ulnar nerve and posterior recurrent ulnar vessels surrounded by fat.
The cubital tunnel is located posterior to the medial epicondyle and contains the ulnar nerve and posterior recurrent ulnar vessels surrounded by fat.
- The medial margins of the trochlea and olecranon form its floor, which is lined by the posterior band of the ulnar collateral ligament. A hypoplastic trochlea can predispose patients to ulnar nerve dislocation. The ulnar collateral ligament relaxes and bulges medially during elbow flexion, which results in narrowing of the cubital tunnel.
- The arcuate ligament forms its roof. This is a fibrous band between the ulnar and humeral heads of the flexor carpi ulnaris muscle and is also known as Osborne's band and the cubital tunnel retinaculum. The arcuate ligament becomes taut with flexion of the elbow. Congenital absence, laxity or a tear of the arcuate ligament can lead to ulnar nerve dislocation.
- The medial epicondyle makes up its anterior border.
The cubital tunnel is the most common site of ulnar nerve compression at the elbow. Cubital tunnel syndrome is due to narrowing of the cubital tunnel or repetitive stress on the ulnar nerve. Elbow flexion in normal subjects results in narrowing of the tunnel by stretching the arcuate ligament; bulging of the medial head of the triceps muscle, which pushes the ulnar nerve anteromedially; and relaxing the ulnar collateral ligament, which bulges medially.
Images through the cubital tunnel during elbow flexion can reveal findings pertinent to cubital tunnel syndrome, including narrowing of the cubital tunnel, attenuation of the perineural fat, bulging of the medial head of the triceps (located more superiorly than the presented slice), and flattening of the ulnar nerve.
Masses in or around the cubital tunnel can cause ulnar nerve compression, including bursae, ganglia, inflammatory synovitis, osteoarthritis, ectopic calcifications, anomalous muscles (e.g., anconeus epitrochlearis) or ligaments (e.g., ligament of Struthers, normally associated with median nerve compression).
Fluid-sensitive sequences often reveal increased signal intensity of the ulnar nerve in the setting of cubital tunnel syndrome.
References
Chapters 2, 10, 11, and 13. In Chung CB and Steinbach LS. MRI of the Upper Extremity: Shoulder, Elbow, Wrist, and Hand. Lippincott Williams & Wilkins. 2010.Monday, November 15, 2010
Os Acromiale
 An os acromiale is an accessory ossification center of the acromion that fails to fuse to the acromion proper by the age of 22 years. The os acromiale may articulate with the acromion by fibrous tissue, cartilage, periosteum, or synovium.
An os acromiale is an accessory ossification center of the acromion that fails to fuse to the acromion proper by the age of 22 years. The os acromiale may articulate with the acromion by fibrous tissue, cartilage, periosteum, or synovium.
Depending on the location of its articulation with the acromion, an os acromiale may be classified as pre-, meso-, meta-, or basi-acromion (see figure).
An os acromiale can be seen in up to 15% of the population, is bilateral in 60% of cases, and may or may not be symptomatic. Most are meso or meta-acromions.
References
Steinbach LS. Chapter 4. In Chung CB and Steinbach LS. MRI of the Upper Extremity: Shoulder, Elbow, Wrist, and Hand. Lippincott Williams & Wilkins. 2010. p 250.Sunday, November 14, 2010
Focal Myocardial Thinning
Differential considerations for focal myocardial thinning:
- Normal Variant: At apex of left ventricle.
- Old myocardial infarction: Thinning restricted to a coronary artery territory and consistent with ECG findings.
- Cardiac sarcoidosis: Most commonly in the septum.
- Muscular left ventricular diverticulum: Tiny crypts in the left ventricular wall that can be seen in normal patients or those with hypertrophic cardiomyopathy.
- Post myocarditis:
- Fibro-fatty replacement:
- Muscular dystrophy: In addition to skeletal muscle involvement, there nearly always is an associated cardiomyopathy in Duchenne or Becker muscular dystrophy.
- Primary aneurysm:
- Dilated phase hypertrophic cardiomyopathy:
- Complete left bundle branch block: Possibly due to redistribution of cardiac mass from chronic asynchronous electric activation.
- Arrhythmogenic right ventricular dysplasia:
References
- Prinzen FW, Cheriex EC, Delhaas T, van Oosterhout MF, Arts T, Wellens HJ, Reneman RS. Asymmetric thickness of the left ventricular wall resulting from asynchronous electric activation: a study in dogs with ventricular pacing and in patients with left bundle branch block. Am Heart J. 1995 Nov;130(5):1045-53.
- Srichai MB, Hecht EM, Kim DC, Jacobs JE. Ventricular diverticula on cardiac CT: more common than previously thought. AJR Am J Roentgenol. 2007 Jul;189(1):204-8.
- Yoshida N, Funabashi N, Uehara M, Yajima R, Kataoka A, Ueda M, Takaoka H, Komuro I. Differentiation of diagnosis and prognoses of non-coronary arterial primary myocardial diseases with left ventricular focal myocardial thinning evaluated by multislice computed tomography. Int J Cardiol. 2009 Nov 3.
Saturday, November 13, 2010
Curvilinear Subpleural Line
 A subpleural line is a thin curvilinear opacity a few millimeters or less in thickness that is usually less than 1 cm from the pleural surface and parallels the pleura.
A subpleural line is a thin curvilinear opacity a few millimeters or less in thickness that is usually less than 1 cm from the pleural surface and parallels the pleura.
This is a nonspecific finding that is classically described in patients with asbestos exposure (as in the case of the patient shown above), in whom the lines are thought to represent the proximal extent of a row of subpleural honeycomb cysts, peribronchiolar fibrosis (and resultant collapse of alveoli), or hypoventilation due to pleural thickening. Dependent subpleural lines can also be seen in normal subjects related to atelectasis.
References
- Aberle DR, Gamsu G, Ray CS. High-resolution CT of benign asbestos-related diseases: clinical and radiographic correlation. AJR Am J Roentgenol. 1988 Nov;151(5):883-91.
- Austin JH, Müller NL, Friedman PJ, Hansell DM, Naidich DP, Remy-Jardin M, Webb WR, Zerhouni EA. Glossary of terms for CT of the lungs: recommendations of the Nomenclature Committee of the Fleischner Society. Radiology. 1996 Aug;200(2):327-31.
- Lynch DA, Gamsu G, Aberle DR. Conventional and high resolution computed tomography in the diagnosis of asbestos-related diseases. Radiographics. 1989 May;9(3):523-51.
Friday, November 12, 2010
Transient Tachypnea of the Newborn
This is a diagnosis of exclusion when no other cause is found for the infant's tachypnea. It is seen in neonates who are sedated or following cesarean section
Radiographs show a normal heart size with findings similar to pulmonary edema: Diffuse, bilateral and usually symmetric increased lung markings. These findings resolve within 1-2 days. Lung volumes may be normal or increased. Pleural effusion and fluid in the fissures may or may not be present.
Differential considerations include:
- Congenital heart disease: Total anomalous pulmonary venous return (TAPVR), severe aortic obstruction (stenosis, coarctation, interruption), hypoplastic left heart
- Meconium aspiration syndrome: Hyperinflated lungs with rope-like perihilar markings
- Neonatal pneumonia:
Thursday, November 11, 2010
Lucent Lesions of the Patella
Differential considerations for lucent lesions of the patella include:
- Dorsal defect of patella: Normal variant
- Subchondral cyst: Can be seen with osteoarthritis or pyrophosphate arthropathy.
- Amyloid deposition: In patients with renal disease.
- Chondroblastoma: Most common benign neoplasm of the patella. Round or lobulated with a well-defined sclerotic rim.
- Giant cell tumor: Geographical pattern of bone destruction. Involve more than 3/4 of the patella and lead to cortical thinning and septations. Locally aggressive
- Pigmented villonodular synovitis:
- Unicameral bone cyst:
- Aneurysmal bone cyst:
- Metastasis:
- Malignant tumor: Hemangioendothelioma, lymphoma, and osteosarcoma.
- Gout: Rare. Soft tissue component may be seen on MRI. Has a predilection for the superolateral aspect of the patella.
- Osteomyelitis: Rare. More common in adolescents (peak vascularity of the patella) or immunocompromised patients. No periosteal reaction (since sesamoids don't have a periosteal layer).
References
Singh J, James SL, Kroon HM, Woertler K, Anderson SE, Jundt G, Davies AM. Tumour and tumour-like lesions of the patella--a multicentre experience. Eur Radiol. 2009 Mar;19(3):701-12.Wednesday, November 10, 2010
Myxopapillary Ependymoma
 Ependymomas are the most common primary spinal cord tumors. They have been classified by the World Health Organization into grades I, II, and III. Grade I tumors include myxopapillary ependymomas and subependymomas. Grade II tumors are just called ependymomas and can be further divided as cellular, papillary, clear cell, or tanycytic. Grade III tumors are called anaplastic ependymomas, tend to occur in the brain, and are rare in the spine.
Ependymomas are the most common primary spinal cord tumors. They have been classified by the World Health Organization into grades I, II, and III. Grade I tumors include myxopapillary ependymomas and subependymomas. Grade II tumors are just called ependymomas and can be further divided as cellular, papillary, clear cell, or tanycytic. Grade III tumors are called anaplastic ependymomas, tend to occur in the brain, and are rare in the spine.
Myxopapillary ependymomas are thought to arise from ependymal glia of the filum terminale and occur almost exclusively in the conus medullaris and filum terminale. As such, they are intradural and usually extramedullary (in contrast to upper cord lesions that are typically intramedullary). Extradural myxopapillary ependymomas, though rare, can also occur and are thought to arise from extradural remnants of the filum terminale or the coccygeal medullary vestige.
Myxopapillary ependymomas are often encapsulated and may have foci of hemorrhagic or mucinous degeneration. They are usually centered within the filum terminale but can extend into the conus medullaris. Myxopapillary ependymomas usually displace the lumbosacral nerve roots, but may encase them if the tumor gets large enough.
Myxopapillary ependymomas are slow-growing and can get large enough to expand the spinal canal, leading to interpedicular widening on frontal radiographs and widening of the spinal canal and scalloped vertebral bodies on the lateral view. Bone destruction may also be appreciated in advanced cases.
Non-contrast CT images reveal myxopapillary ependymomas to be isoattenuating compared to the spinal cord. The spinal canal may be widened and there may be scalloping of the vertebral bodies with neural foraminal enlargement. Myxopapillary ependymomas typically have intense homogeneous enhancement.
On MRI, myxopapillary ependymomas are typically iso- to hyperintense compared to the spinal cord on T1-weighted images, depending on the amount of proteinaceous mucoid matrix. If present, T1-hyperintensity helps differentiate myxopapillary ependymomas from other ependymoma subtypes, which tend to be hypo- or isointense on T1-weighted images. Myxopapillary ependymomas are T2-hyperintense compared to the spinal cord. As with other ependymomas, myxopapillary ependymomas demonstrate intense enhancement. Heterogeneous enhancement signifies hemorrhage or necrosis.
Most ependymomas of the cauda equina region are slow-growing, and patients present with indolent low back pain. Mass effect from the tumor may cause sciatica or other, less common symptoms, such as sensorimotor disturbance and bowel and bladder dysfunction.
Differential considerations include:
- Other ependymoma subtypes:
- Schwannoma: Can have findings almost identical to those of a small myxopapillary ependymoma.
- Subependymoma: Can have findings almost identical to those of a small myxopapillary ependymoma.
- Astrocytoma:
- Hemangioblastoma:
- Ganglioma:
- Paraganglioma:
Our patient was a young man who presented with several years of low back and flank pain. A renal tumor protocol CT was performed, which showed a mass in the spinal canal. On MR, the mass is well encapsulated, isointense to the spinal cord on T1-weighted images and heterogeneously hyperintense on T2-weighted images. Post-contrast images reveal intense heterogeneous enhancement. On the axial T2-weighted image, the mass splays the nerve roots of the cauda equina and widens the spinal canal.
Case courtesy of Dr. Sibin Thachet.
References
- Shors SM, Jones TA, Jhaveri MD, Huckman MS. Best cases from the AFIP: myxopapillary ependymoma of the sacrum. Radiographics. 2006 Oct;26 Suppl 1:S111-6.
- Wippold FJ 2nd, Smirniotopoulos JG, Moran CJ, Suojanen JN, Vollmer DG. MR imaging of myxopapillary ependymoma: findings and value to determine extent of tumor and its relation to intraspinal structures. AJR Am J Roentgenol. 1995 Nov;165(5):1263-7.
Tuesday, November 9, 2010
Wall-to-wall Cardiothymic Silhouette in Neonates
- Ebstein anomaly: Massive right atrial enlargement. Decreased pulmonary blood flow.
- Pulmonary atresia with intact ventricular septum: Massive right atrial enlargement. Decreased pulmonary blood flow.
- Large pericardial effusion: Seen in hydrops fetalis, sepsis, cardiac tumors, thyroid dysfunction, and diaphragmatic hernia into the pericardial sac.
- Atypical large arteriovenous shunts: For example, peripheral arteriovenous malformations or intracardiac arteriovenous malformations (e.g., coronary artery-right heart fistula). Pulmonary vascularity may be normal due to the high pulmonary vascular resistance of newborns.
- Hypertrophic cardiomyopathy in infants of diabetic mothers:
- Cardiac or mediastinal mass mimicking massive cardiomegaly: Rhabdomyoma (e.g., in children with tuberous sclerosis), teratomas, and congenital diaphragmatic hernia (before gas enters the bowel).
References
Donnelly LF, Gelfand KJ, Schwartz DC, Strife JL. The wall to wall heart: Massive cardiothymic silhouette in newborns. Applied Radiology. 1997 December; 26(12).Monday, November 8, 2010
Shunt Vascularity
Shunt vascularity refers to increased number and size of sharply defined pulmonary vessels (in contrast to blurred vessels seen in pulmonary edema) in response to diversion of blood to the lungs. There is no or minimal tapering of these enlarged vessels, especially in the upper lungs (in contrast to the pruning seen in pulmonary hypertension).
The most common causes of shunt vascularity are:
The most common causes of shunt vascularity are:
- Left-to-right: Acyanotic.
- Atrial septal defect: The left atrium is not enlarged. No significant cardiomegaly unless a complicated atrial septal defect exists.
- Partial anomalous pulmonary venous return: Some pulmonary veins drain into the right atrium or systemic veins instead of the left atrium. The left atrium is not enlarged, but cardiomegaly may occur if the left-to-right shunt is significant.
- Ventricular septal defect: Cardiomegaly with an enlarged left atrium and main pulmonary artery.
- Patent ductus arteriosus: Enlarged left atrium. May see a prominent aortic knob.
- Endocardial cushion defect: Strong association with Trisomy 21. The heart may be enlarged.
Simplistic view for boards purposes:

- Mixed: Cyanotic
- Total anomalous pulmonary venous return: Normal-sized heart.
- Complete transposition of the great vessels: Egg-on-a-string. Classically described as thymic atrophy and an enlarged heart with an oval-shape and an upturned apex. The position of the aorta and pulmonary trunk results in a narrow superior mediastinum. Together, the upturned heart and narrow mediastinum result in the egg-on-a-string appearance.
- Persistent truncus arteriosus: A single-vessel carries outflow from the heart, overrides the ventricular septum, and supplies the systemic, pulmonary, and coronary circulation. The heart is enlarged and there is frequently a right-sided aortic arch.
- Hypoplastic left heart: Oxygenated blood passes to the right side via an atrial septal defect, and mixed blood travels to the aorta via a patent ductus arteriosus. Typically will see an enlarged heart with a prominent right atrium.
- Single ventricle: Double outlet right ventricle and double outlet left ventricle are conceptually similar.
- High-flow state:
- Arteriovenous malformation: Vein of Galen malformation, for example.
- Anemia:
- Thyrotoxicosis:

References
- Bardo DM, Frankel DG, Applegate KE, Murphy DJ, Saneto RP. Hypoplastic left heart syndrome. Radiographics. 2001 May-Jun;21(3):705-17.
- Bardo DM, Frankel DG, Applegate KE, Murphy DJ, Saneto RP. Hypoplastic left heart syndrome. Radiographics. 2001 May-Jun;21(3):705-17.
- Daffner RH. Clinical radiology: the essentials. Lippincott Williams & Wilkins, 2007.
Sunday, November 7, 2010
Rectal Duplication
 Rectal duplications are rare anomalies that may be lined with colonic (most common), squamous epithelium, gastric mucosa, and urothelial cells. The vast majority are retrorectal. Rectal duplications may be classified as:
Rectal duplications are rare anomalies that may be lined with colonic (most common), squamous epithelium, gastric mucosa, and urothelial cells. The vast majority are retrorectal. Rectal duplications may be classified as:
- Tubular: Associated with urinary or vertebral malformations.
- Cystic: Associated with anorectal malformations, such as anterior perineal anus and cloacal malformations.
- Fistulated (internal or external):
- Diverticular:
- Exstrophic: May be attached to the rectum or vagina, but does not normally communicate with either.
References
Rajah S, Ramanujam TM, Anas SR, Jayaram G, Baskaran P, Ganesan J, Tin M. Duplication of the rectum: report of four cases and review of the literature. Pediatr Surg Int. 1998 Jul;13(5-6):373-6.Saturday, November 6, 2010
The Celery Stalk Sign
 The celery stalk sign refers to the appearance of hyperintense bands interposed between the fibers of a normally oriented anterior cruciate ligament (ACL). The celery stalk is best appreciated on sagittal, fluid-sensitive sequences. The hyperintense bands correspond to amorphous mucoid matrix collecting between intact, almost parallel anterior cruciate ligament fibers.
The celery stalk sign refers to the appearance of hyperintense bands interposed between the fibers of a normally oriented anterior cruciate ligament (ACL). The celery stalk is best appreciated on sagittal, fluid-sensitive sequences. The hyperintense bands correspond to amorphous mucoid matrix collecting between intact, almost parallel anterior cruciate ligament fibers.
The celery stalk appearance corresponds to mucoid degeneration of the anterior cruciate ligament and should not be mistaken for a chronic or acute tear.
The celery stalk sign should not be confused with the celery stalk metaphysis.
References
Papadopoulou P. The celery stalk sign. Radiology. 2007 Dec;245(3):916-7.Friday, November 5, 2010
Infrequent Voiding Syndrome
 Infrequent voiding syndrome, also known as lazy bladder syndrome, refers to the constellation of findings in patients who voluntarily delay voiding, resulting in large-capacity urinary bladders with weak or absent detrussor contractile function. Patients may present with urinary leakage, urinary tract infections, abdominal pain, palpable pelvic mass, increased work of voiding and a weak urinary stream, or constipation.
Infrequent voiding syndrome, also known as lazy bladder syndrome, refers to the constellation of findings in patients who voluntarily delay voiding, resulting in large-capacity urinary bladders with weak or absent detrussor contractile function. Patients may present with urinary leakage, urinary tract infections, abdominal pain, palpable pelvic mass, increased work of voiding and a weak urinary stream, or constipation.
Voiding cystourethrogram reveals an enlarged and smooth-walled urinary bladder, with a large post-void residual. Scout views may reveal a large amount of fecal material.
The case presented here is from a teenager with frequent urinary tract infections. The scout view shows a moderate amount of stool in the colon. We see a large (500-cc capacity), smooth-walled urinary bladder with a small right-sided diverticulum (arrow) and no significant post-void residual.
A rough guide for determining normal urinary bladder volumes:

You can then multiply by 30 to get a rough estimate in normal (SI) units.
Equations made with the online LaTeX equation editor.
References
- Kaefer M, Zurakowski D, Bauer SB, Retik AB, Peters CA, Atala A, Treves ST. Estimating normal bladder capacity in children. J Urol. 1997 Dec;158(6):2261-4.
- Lalli AF, Thornbury JR, Lapides J. Large capacity smooth-walled bladders as an indication of the infrequent voiding syndrome. J Urol. 1971 May;105(5):662-3.
Thursday, November 4, 2010
Extralobar Pulmonary Sequestration with Torsion
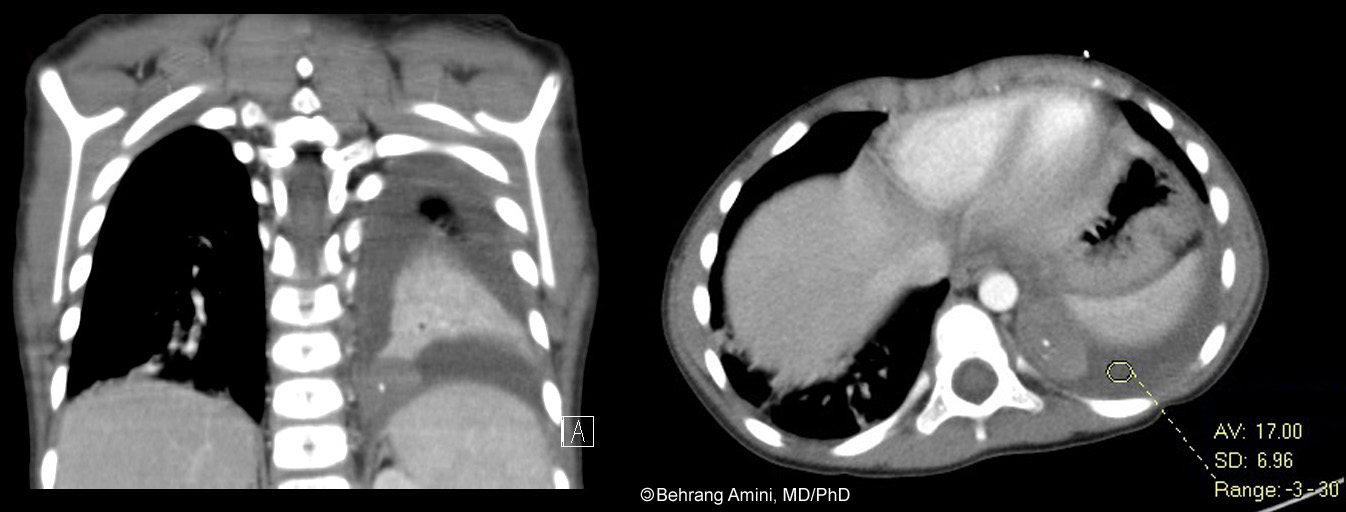 Pulmonary sequestration refers to the presence of a mass of abnormal lung tissue that does not communicate with the tracheobronchial tree through normally located bronchi and has blood supply through anomalous systemic arteries.
Pulmonary sequestration refers to the presence of a mass of abnormal lung tissue that does not communicate with the tracheobronchial tree through normally located bronchi and has blood supply through anomalous systemic arteries.
Pulmonary sequestrations can be classified as intralobar or extralobar depending on their pleural investment, with intralobar sequestrations located within the same visceral pleura as the normal lung and extralobar sequestrations located outside the lung with their own pleural investment. Intralobar sequestrations may have systemic or pulmonary drainage, while extralobar sequestrations have systemic venous drainage. As mentioned above, both have systemic arterial supply.
Patients with intralobar sequestrations usually can present in adulthood with recurrent infections, hemoptysis, and respiratory distress. Patients with extralobar sequestration are usually diagnosed in infancy or childhood on chest radiographs obtained for other reasons, possibly for associated cardiac or other congenital anomalies.
An unusual presentation of extralobar sequestration is torsion and infarction sometimes with a pleural effusion (hemorrhagic or bland). As expected with an infarcted organ, patients present with chest pain.
Our patient presented with 6 days of abdominal pain with progressive shortness of breath, pleuritic chest pain, and hypoxia with exertion. We see a pleural effusion with attenuation of about 20. There is also a posteromedial mass with a focal calcification. The mass doesn't enhance as much as the rest of the adjacent collapsed lung. During surgery, a torsed artery was seen extending through the diaphragm to the mass (the artery was not seen on imaging). Pathology revealed an infarcted extralobar sequestration.
References
- Huang EY, Monforte HL, Shaul DB. Extralobar pulmonary sequestration presenting with torsion. Pediatr Surg Int. 2004 Mar;20(3):218-20.
- Lima M, Randi B, Gargano T, Tani G, Pession A, Gregori G. Extralobar pulmonary sequestration presenting with torsion and associated hydrothorax. Eur J Pediatr Surg. 2010 May;20(3):208-10.
- Mammen A, Myers NA, Beasley SW. Torsion and infarction of an extralobar pulmonary sequestration: A rare cause of haemorrhagic pleural effusion. Pediatr Surg Int. 1994 9(5-6):399-400.
- Shah R, Carver TW, Rivard DC. Torsed pulmonary sequestration presenting as a painful chest mass. Pediatr Radiol. 2010 Aug;40(8):1434-5.
Wednesday, November 3, 2010
Collateral Pathways from the Aorta to the Lower Extremities
Collateral pathways exist for arterial blood to reach the lower extremities when the infrarenal aorta is occluded.
- Anterior (Winslow) pathway: subclavian arteries to internal mammary arteries. Internal mammary arteries to superior epigastric arteries. Superior epigastric arteries to the inferior epigastric arteries. Inferior epigastric arteries to the external iliac arteries.
- Middle (visceral) pathway: Superior mesenteric artery to inferior mesenteric artery via the marginal artery of Drummond (marginal artery of the colon) and the arcade of Riolan (intestinal arterial arcade). Inferior mesenteric artery to superior hemorrhoidal artery. Superior hemorrhoidal artery to middle and inferior hemorrhoidal arteries. Middle and inferior hemorrhoidal arteries to the external iliac arteries.
- Posterior pathway (1): Intercostal, subcostal, and lumbar arteries to the superior gluteal and iliolumbar arteries. Superior gluteal and iliolumbar arteries to the internal iliac arteries. Internal iliac arteries to the external iliac arteries.
- Posterior pathway (2): Intercostal, subcostal, and lumbar arteries to the superficial and deep iliac circumflex arteries. Circumflex arteries to the external iliac arteries.
References
- Prager RJ, Akin JR, Akin GC, Binder RJ. Winslow's pathway: a rare collateral channel in infrarenal aortic occlusion. AJR Am J Roentgenol. 1977 Mar;128(3):485-7.
- Sebastià C, Quiroga S, Boyé R, Perez-Lafuente M, Castellà E, Alvarez-Castells A. Aortic stenosis: spectrum of diseases depicted at multisection CT. Radiographics. 2003 Oct;23 Spec No:S79-91.
Tuesday, November 2, 2010
Supracristal Ventricular Septal Defect
A supracristal (also known as subpulmonic or doubly committed) ventricular septal defect (VSD) lies above the crista supraventricularis and below the pulmonic valve, such that the aortic and pulmonary valves are in fibrous continuity.
Supracristal ventricular septal defects are the least common of the VSDs, comprising between 2%-3% of cases. They are hard to detect on echocardiography, but have a typical appearance on angiography and MRI.
On angiograms in the frontal projection, a jet of contrast material can be seen passing from the left ventricle beneath the left aspect of the aortic valve into the outflow tract of the right ventricle just below the pulmonary valve.
Axial MR images at the level of the right ventricular outflow tract reveal a defect between the base of the aorta and the upper posterior aspect of the right ventricular infundibulum. Cine MRI will a flow jet in the distal right ventricular outflow tract into the main pulmonary artery.
Supracristal ventricular septal defects are seen in is association with:
Supracristal ventricular septal defects are the least common of the VSDs, comprising between 2%-3% of cases. They are hard to detect on echocardiography, but have a typical appearance on angiography and MRI.
On angiograms in the frontal projection, a jet of contrast material can be seen passing from the left ventricle beneath the left aspect of the aortic valve into the outflow tract of the right ventricle just below the pulmonary valve.
Axial MR images at the level of the right ventricular outflow tract reveal a defect between the base of the aorta and the upper posterior aspect of the right ventricular infundibulum. Cine MRI will a flow jet in the distal right ventricular outflow tract into the main pulmonary artery.
Supracristal ventricular septal defects are seen in is association with:
- Aortic regurgitation
- Balloon-like dilatation of the right coronary sinus
- Prolapse of the right coronary cusp into the right ventricular infundibulum
- Right coronary sinus-right ventricular fistula
- Double outlet right ventricle with supracristal ventricular septal defect (Taussig-Bing anomaly).
References
- Bremerich J, Reddy GP, Higgins CB. MRI of supracristal ventricular septal defects. J Comput Assist Tomogr. 1999 Jan-Feb;23(1):13-5.
- Jaffe RB, Scherer JS. Supracristal ventricular septal defects: spectrum of associated lesions and complications. AJR Am J Roentgenol. 1977 Apr;128(4):629-37.
- Miller LR, Nemeth M, Flamm SD, Sung C, Stainback RF. Supracristal ventricular septal defect. Tex Heart Inst J. 2006;33(1):96-7.
Monday, November 1, 2010
Grading of Systolic Anterior Motion

Systolic anterior motion (SAM) can be graded by echocardiography based on the contact between the mitral valve leaflet and septum during systole.
- Grade I (mild): No contact between the mitral valve leaflet and septum with a minimum separation > 10 mm.
- Grade II (moderate): No contact between the mitral valve leaflet and septum with a minimum separation < 10 mm OR contact between the mitral valve leaflet and septum lasting < 30% of systolic time.
- Grade III (severe) : Contact between the mitral valve leaflet and septum lasting > 30% of systolic time.
References
Gilbert BW, Pollick C, Adelman AG, Wigle ED. Hypertrophic cardiomyopathy: subclassification by m mode echocardiography. Am J Cardiol. 1980 Apr;45(4):861-72.
Subscribe to:
Posts (Atom)