 Pulmonary sequestration refers to the presence of a mass of abnormal lung tissue that does not communicate with the tracheobronchial tree through normally located bronchi and has blood supply through anomalous systemic arteries.
Pulmonary sequestration refers to the presence of a mass of abnormal lung tissue that does not communicate with the tracheobronchial tree through normally located bronchi and has blood supply through anomalous systemic arteries.
Pulmonary sequestrations can be classified as intralobar or extralobar depending on their pleural investment, with intralobar sequestrations located within the same visceral pleura as the normal lung and extralobar sequestrations located outside the lung with their own pleural investment. Intralobar sequestrations may have systemic or pulmonary drainage, while extralobar sequestrations have systemic venous drainage. As mentioned above, both have systemic arterial supply.
Patients with intralobar sequestrations usually can present in adulthood with recurrent infections, hemoptysis, and respiratory distress. Patients with extralobar sequestration are usually diagnosed in infancy or childhood on chest radiographs obtained for other reasons, possibly for associated cardiac or other congenital anomalies.
An unusual presentation of extralobar sequestration is torsion and infarction sometimes with a pleural effusion (hemorrhagic or bland). As expected with an infarcted organ, patients present with chest pain.
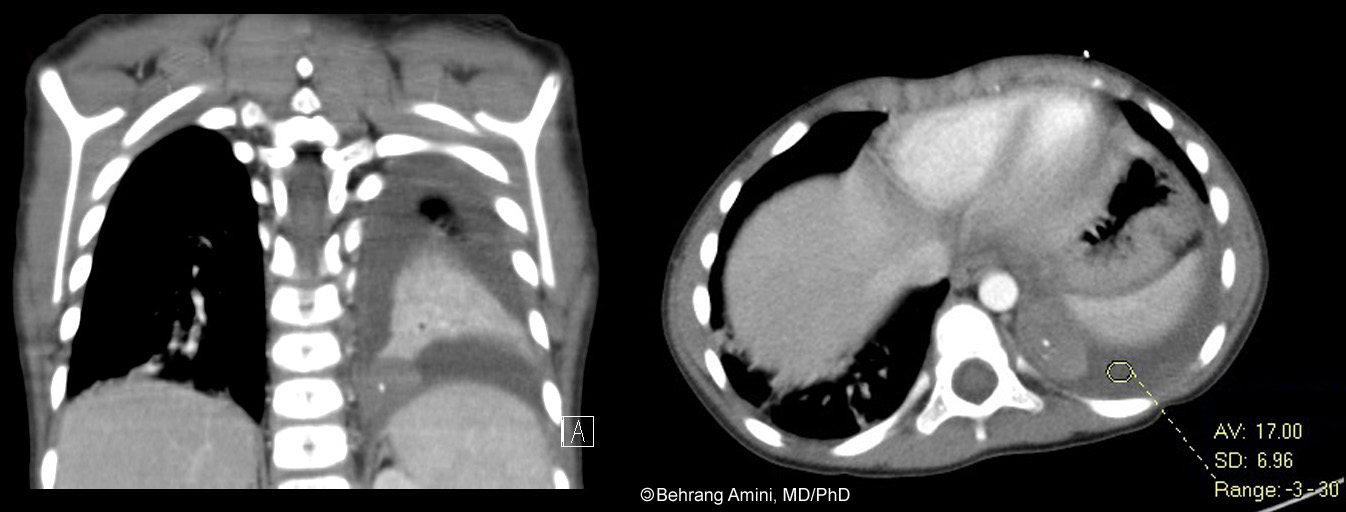
Our patient presented with 6 days of abdominal pain with progressive shortness of breath, pleuritic chest pain, and hypoxia with exertion. We see a pleural effusion with attenuation of about 20. There is also a posteromedial mass with a focal calcification. The mass doesn't enhance as much as the rest of the adjacent collapsed lung. During surgery, a torsed artery was seen extending through the diaphragm to the mass (the artery was not seen on imaging). Pathology revealed an infarcted extralobar sequestration.
References
- Huang EY, Monforte HL, Shaul DB. Extralobar pulmonary sequestration presenting with torsion. Pediatr Surg Int. 2004 Mar;20(3):218-20.
- Lima M, Randi B, Gargano T, Tani G, Pession A, Gregori G. Extralobar pulmonary sequestration presenting with torsion and associated hydrothorax. Eur J Pediatr Surg. 2010 May;20(3):208-10.
- Mammen A, Myers NA, Beasley SW. Torsion and infarction of an extralobar pulmonary sequestration: A rare cause of haemorrhagic pleural effusion. Pediatr Surg Int. 1994 9(5-6):399-400.
- Shah R, Carver TW, Rivard DC. Torsed pulmonary sequestration presenting as a painful chest mass. Pediatr Radiol. 2010 Aug;40(8):1434-5.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.