- Hyperuricemia from purine metabolism
- Hyperkalemia
- Hyperphosphatemia
- Hypocalcemia caused by hyperphosphatemia and the resultant precipitation of calcium phosphate.
The Cairo-Bishop definition includes two classes of tumor lysis syndrome:
Laboratory tumor lysis syndrome: Any 2 of the following:
- Uric acid > 8 mg/dL or 25% increase
- Potassium > 6 mEq/L or 25% increase
- Phosphate > 4.5 mg/dL or 25% increase
- Calcium < 7 mg/dL or 25% decrease
- Creatinine > 1.5x upper limit of normal
- Seizure
- Cardiac arrhythmia
- Sudden death
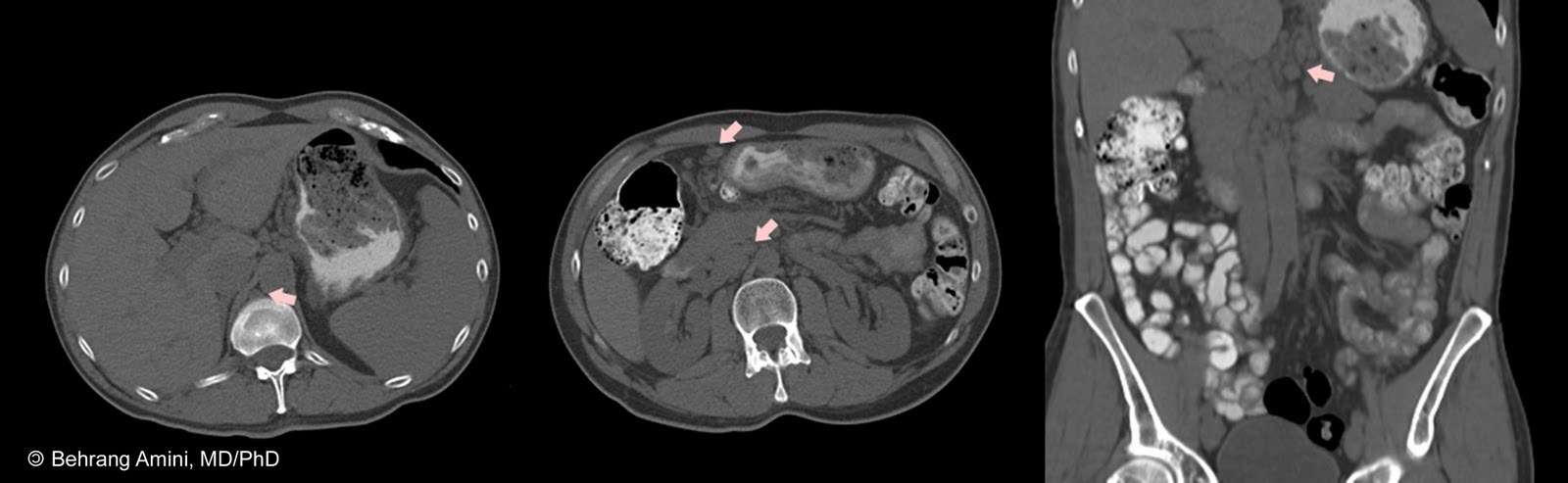
Imaging findings can include nephromegaly, renal stone formation with obstructive uropathy, and findings of posterior reversible encephalopathy syndrome (PRES).
References
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004 Oct;127(1):3-11.
- Kaito E, Terae S, Kobayashi R, Kudo K, Tha KK, Miyasaka K. The role of tumor lysis in reversible posterior leukoencephalopathy syndrome. Pediatr Radiol. 2005 Jul;35(7):722-7.
- Lehner SG, Gould JE, Saad WE, Brown DB. Tumor lysis syndrome after radiofrequency ablation of hepatocellular carcinoma. AJR Am J Roentgenol. 2005 Nov;185(5):1307-9.
- Parisi MT, Fahmy JL, Kaminsky CK, Malogolowkin MH. Complications of cancer therapy in children: a radiologist's guide. Radiographics. 1999 Mar-Apr;19(2):283-97.