
Sarcoidosis typically presents with lung involvement; however, abdominal viscera are frequently involved as well.
- Liver: Most common imaging abnormality is hepatomegaly (30%). May also have multiple low-attenuation intrahepatic septa on contrast-enhanced CT; multiple low-attenuation, low-intensity (on all sequences), and poorly enhancing nodules nodules.
- Bile ducts: Involvement of intrahepatic bilde ducts can result in a cholestatic picture, mimicking that of primary biliary cirrhosis. Involvement of the extrahepatic ducts can produce strictures that mimic cholangiocarcinoma, while enlargement of portal lymph nodes can compress the biliary tree to produce obstructive jaundice.
- Spleen: Splenomegaly is seen in about 30%. Low-attenuation/intensity (on all pulse sequences) splenic nodules are seen in 5% - 30% of patients. Isolated/predominant nodular splenic disease is more common than isolated/predominant hepatic nodular disease. Punctate calcifications may also be seen.
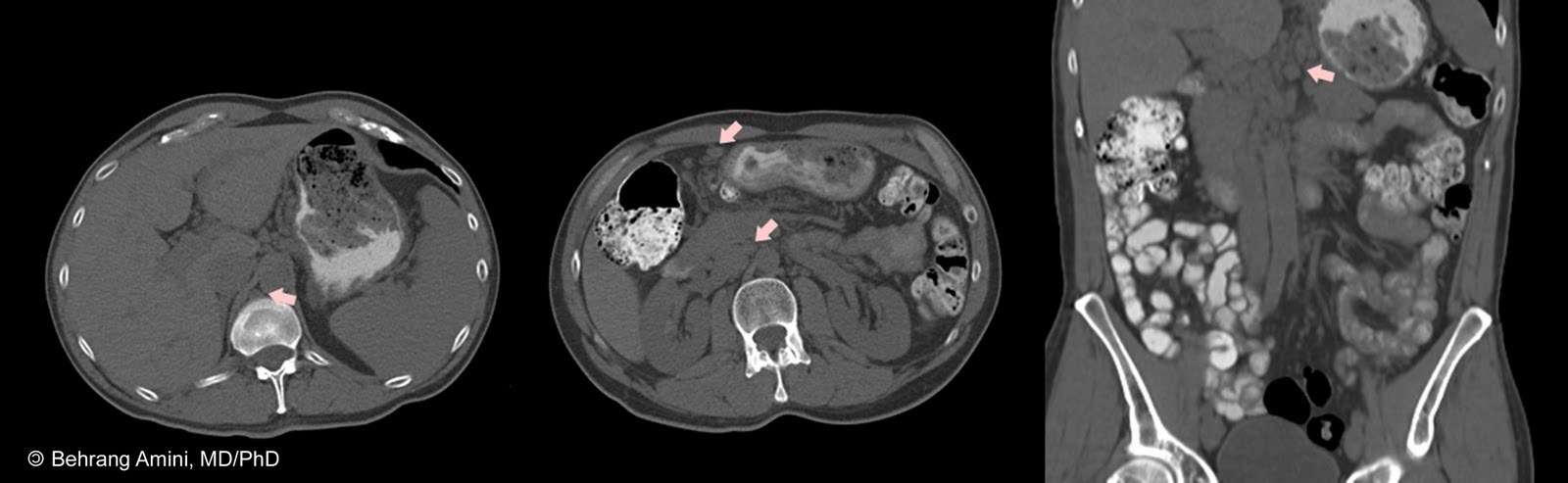
- Lymph nodes: Our patient's only manifestation of sarcoidosis on the unenhanced CT was adbominal adenopathy. In fact, one study found that abdominal adenopathy was the only abnormal finding in approximately 50% of patients in one study.
Abdominal adenopathy is seen in about 30% of patients. Nodal calcification is unusual in sarcoidosis. The main differential, lymphoma, has essentially the same distribution of adenopathy, although retrocrural lymph nodes are seen more frequently (70%) in patients with lymphoma compared to those with sarcoidosis (20%). Our patient had retrocrural, retroperitoneal, and mesenteric adenopathy, and lymphoma was considered as a possibility.
- Pancreas: Direct pancreatic involvement is uncommon, but may result in diabetes or pancreatitis. Sarcoid-associated hypercalcemia may also result in acute pancreatitis.
- Kidneys: While the kidney is involved in 5%-20% of cases at autopsy, a radiographically detectable renal mass is unusual. Nephromegaly or renal atrophy may be the only manifestation. The appearance of granulomas in renal sarcoid is similar to that previously described for the liver and the spleen. The main differential considerations are lymphoma and metastasis.
The most common effect of renal sarcoidosis is hypercalciuria (more common) or hypercalcemia, which may result in nephrocalcinosis, nephrolithiasis, and interstitial calcium deposition. However, radiographically detectable nephrocalcinosis is uncommon, having been reported in 1%–4% of patients. The mechanism is increased conversion of 25-hydroxyvitamin D3 to active 1,25 dihydroxyvitamin D by macrophages in granulomas, resulting in increased intestinal calcium absorption.
An interesting result of this disturbance in calcium metabolism is the effect of sunlight. Acute sunlight exposure can precipitate hypercalcemia in this setting, resulting in malaise, dehydration, or acute pancreatitis.
- Gastrointestinal Tract: Radiographically visible involvement of the gastrointestinal tract appears to be uncommon, with appearances ranging from plaques and ulcers to linear and polypoid filling defects. The stomach is most commonly affected, where involvement can result in mucosal nodularity and thickened irregular folds that mimics Ménétrier disease, or a linitis plastica appearance that can mimic gastric adenocarcinoma.
References
Warshauer DM, Lee JK. Imaging manifestations of abdominal sarcoidosis. AJR Am J Roentgenol. 2004 Jan;182(1):15-28.
 Sarcoidosis typically presents with lung involvement; however, abdominal viscera are frequently involved as well.
Sarcoidosis typically presents with lung involvement; however, abdominal viscera are frequently involved as well.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.