POEMS syndrome is a paraneoplastic syndrome related to a plasma cell dyscrasia that is also known as Crow-Fukase syndrome, Takatsuki syndrome. The acronyms POEMS (Polyneuropathy, Organomegaly, Endocrinopathy, M protein and Skin changes) and PEP (Plasma cell dyscrasia, Endocrinopathy and Polyneuropathy), capture some—but not all—of the associated manifestations. Other manifestations include sclerotic bone lesions, Castleman disease, papilledema, thrombocytosis, erythrocytosis, pleural effusions, edema, and ascites.
Given this potential variability in presentation, Dispenzieri et al. proposed major and minor criteria for the diagnosis of POEMS syndrome. The major criteria are polyneuropathy and monoclonal plasmaproliferative disorder.
Minor criteria include sclerotic bone lesions, Castleman disease, Organomegaly (splenomegaly, hepatomegaly, or lymphadenopathy), Edema (edema, pleural effusion, or ascites), endocrinopathy (adrenal, thyroid, pituitary, gonadal, parathyroid, pancreatic), skin changes (hyperpigmentation, hypertrichosis, plethora, hemangiomata, white nails), papilledema.
They proposed that two major criteria and at least one minor criterion differentiate POEMS syndrome from neuropathy associated with monoclonal gammopathy of undetermined significance, myeloma, and Waldenström disease.
The vast majority of POEMS syndrome patients have radiographic evidence of bone lesions at presentation. Slightly less than half of these lesions are purely sclerotic (well-defined or fluffy), approximately half are mixed sclerotic and lytic, and a small number (2%) are purely lytic bone lesions, which tend to have scelrotic margins giving them a
unique ring-like appearance. More than half of patients with bone lesions had more than one lesion.
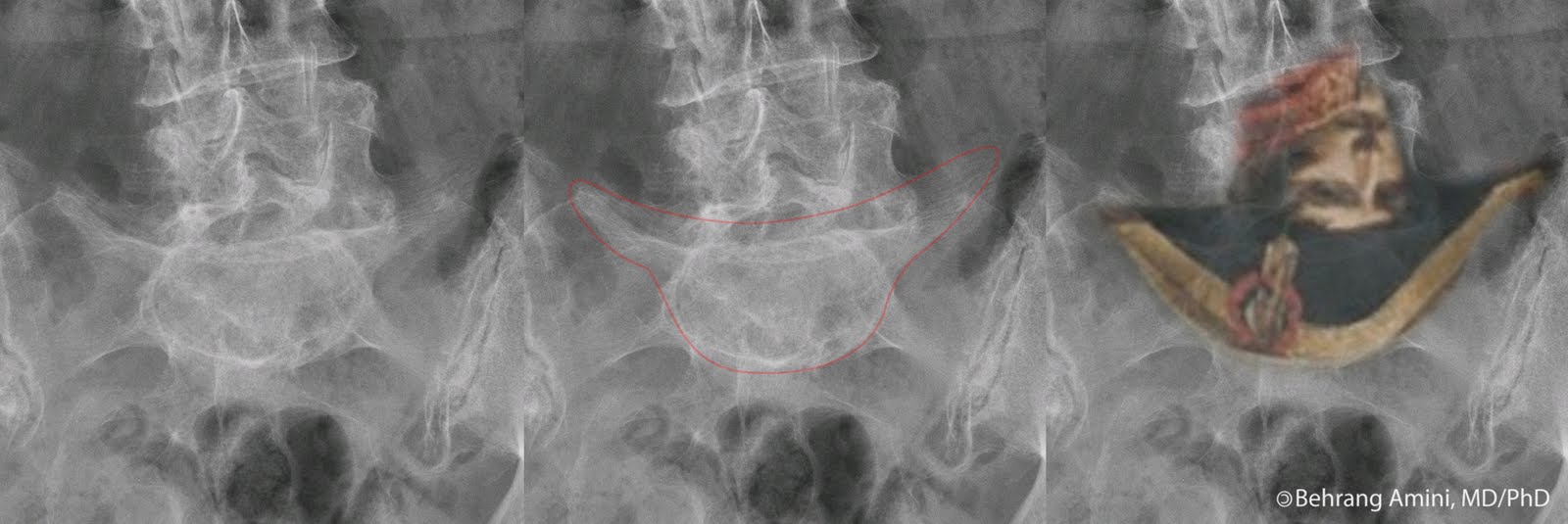
Resnick has described a pattern of bony proliferation that is pathognomonic for POEMS syndrome: irregular and spiculated bone contours at areas of tendinous and ligamentous attachment, posterior elements of the spine (facet joints, laminae, transverse processes, and costovertebral articulations).
Differential considerations for the sclerotic bone lesions include:
Differential considerations for the proliferative spine lesions include:
- Diffuse idiopathic skeletal hyperostosis (DISH): Also has flowing anterior ossifications.
- Seronegative spondyloarthropathy: Look for syndesmophytes, sacroiliac joint ankylosis.
- Fluorosis: Also has increased bone density.
- Hypoparathyroidism:
- X-linked hypophosphatemia:
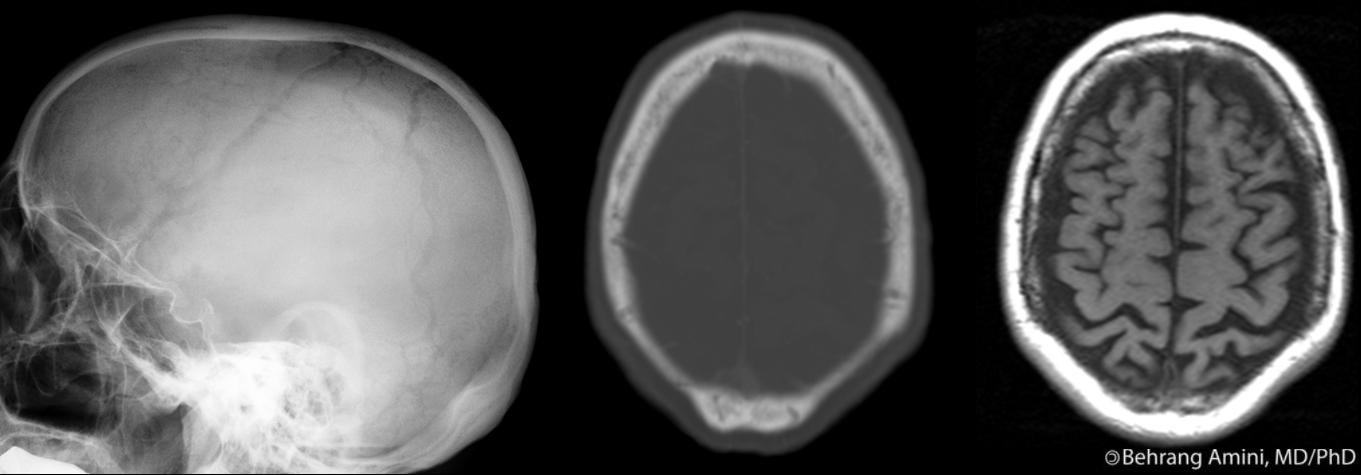
The images above are from a patient with POEMS syndrome. We see sclerotic lesions in the humerus, pelvis, and proximal femur, some of which have the typical ring-like appearance (e.g., the left intertrochanteric region). Looking through our 20 or so cases of POEMS here, I wasn't able to find any with the pathognomonic proliferative changes described by Resnick, so a look at the original paper is worthwhile to get familiar with this appearance.
Special thanks to Dr. James Dimaala for the case.
References
- Chong ST, Beasley HS, Daffner RH. POEMS syndrome: radiographic appearance with MRI correlation. Skeletal Radiol. 2006 Sep;35(9):690-5.
- Dispenzieri A, Kyle RA, Lacy MQ, Rajkumar SV, Therneau TM, Larson DR, Greipp PR, Witzig TE, Basu R, Suarez GA, Fonseca R, Lust JA, Gertz MA. POEMS syndrome: definitions and long-term outcome. Blood. 2003 Apr 1;101(7):2496-506.
- Owens CL, Weir EG, Ali SZ. Cytopathologic findings in "POEMS" syndrome associated with Castleman disease. Diagn Cytopathol. 2007 Aug;35(8):512-5.
- Resnick D, Greenway GD, Bardwick PA, Zvaifler NJ, Gill GN, Newman DR. Plasma-cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M-protein, and skin changes: the POEMS syndrome. Distinctive radiographic abnormalities. Radiology. 1981 Jul;140(1):17-22.
 The Yune soft tissue index is used to assess the amount of soft tissue at the tips of the distal phalanges. This can help in early detection of acral soft-tissue atrophy (for example, in patients with scleroderma).
The Yune soft tissue index is used to assess the amount of soft tissue at the tips of the distal phalanges. This can help in early detection of acral soft-tissue atrophy (for example, in patients with scleroderma).